A new study shows the sugar sialic acid, which makes up part of the protective intestinal mucus layer, fuels disease-causing bacteria in the gut. The findings, published in PNAS, suggest a potential treatment target for intestinal bacterial infections and a range of chronic diseases linked to gut bacteria, including inflammatory bowel disease (IBD), celiac disease, irritable bowel syndrome and short bowel syndrome.
The research by researchers at the University of British Columbia (UBC) and BC Children’s Hospital, used a mouse model of gut infections.
“Bacteria need to find a place in our intestines to take hold, establish and expand, and then they need to overcome all the different defences that normally protect our gut,” says Dr Bruce Vallance, a professor in the department of paediatrics at UBC and investigator at BC Children’s Hospital. “In the future, we can potentially target this sugar, or how pathogens sense it, to prevent clinically important disease.”
Inflammatory diseases such as IBD are on the rise in children, who are more susceptible to gut infections because of their immature immune systems. Dr Vallance and his team sought to understand what enables these bacterial pathogens to survive and expand inside our intestines.
For the study, the researchers examined Citrobacter rodentium, an intestinal bacterial pathogen of mice that’s used to model infections with human E. coli. The team discovered that the bacteria have genes involved in sialic acid consumption, and when these genes are removed, the bacteria’s growth is impaired.
Further investigation revealed that upon consuming the sugars, the bacteria produced two special virulence proteins that help the bacteria cross the colonic mucus layer and stick to the underlying epithelial cells. The findings reveal how the bacteria can change over time and actually worsen disease.
“You start off with IBD, your microbes change, they start digging their way into the cells lining your gut, causing more inflammation, and that may be one reason why IBD becomes chronic,” says Dr Vallance. “Specific nutrients such as sialic acid or other sugars might be the Achilles heels for them in terms of things you could target to remove dangerous bacteria from the intestine.”
Dr Vallance and his team are now examining the role other sugars in the gut may play in feeding pathogenic bacteria. They’re also looking for probiotics that could outcompete the dangerous bacteria, stealing the sugars away from them.
They also plan to explore potential interactions between resident and pathogenic bacteria. Pathogenic bacteria can’t access the sugars on their own and thus, some of the normally harmless resident bacteria must serve as accomplices.
“Basically, these accomplices cut the sugar off the mucus, and then either they hand it to the dangerous bacteria or the dangerous bacteria have come up with a way of stealing it from them,” he explains.
A better understanding of these interactions could provide new ways to block pathogenic bacteria, something Dr. Vallance says is urgently needed.
“In the past, our ancestors were constantly assaulted by dangerous bacteria,” says Dr. Vallance. “With the advent of more and more antibiotic resistance in bacteria, these bacterial infections are going to become a growing problem again. Without new antibiotics, we need to come up with novel ways to fight these bacteria, like starving them.”
Several sessions at the 11th SA AIDS conference, recently held in Durban, highlighted the worrying fact that key HIV numbers such as treatment coverage are much lower in children than in adults. There is hope, however, that new treatments and new treatment guidelines might help close the gap.
In a plenary session, Dr Sandile Buthelezi, Director General of the National Department of Health, told delegates that on UNAIDS’ 95-95-95 targets, children in South Africa are at 81-65-68. This means that 81% of children living with HIV have been diagnosed, 65% of those diagnosed are on antiretroviral treatment, and 68% of those on treatment are virally suppressed. For the South African population as a whole, the numbers are at 94-76-92.
Throughout the conference, various speakers highlighted the fact that only 65% of children who have been diagnosed are on treatment as a particular concern. To close the gap and reach UNAIDS’ target of 95%, just over an additional 88 000 children would need to be initiated on treatment.
Professor Lee Fairlie, Director of Maternal and Child Health at Wits RHI, said in a presentation that only 52% of children younger than 14 living with HIV are on treatment. Fairlie also pointed out that children lagged behind substantially when it comes to viral suppression, and this is particularly challenging in the youngest age groups.
Not all bad news
But it was not all bad news at this year’s conference. One piece of good news is that new and better child-friendly antiretroviral formulations are being rolled out in South Africa. These new treatments should make it easier for children to start and stay on treatment – children often find it difficult to take medicines formulated for adults, due to factors like incorrect dosing, large pills, and bad taste.
The National Department of Health recently updated the country’s antiretroviral treatment guidelines to allow for the use of several of these new formulations and better HIV treatment regimens for children. Most notable is the introduction of a new regimen consisting of the medicines abacavir, lamivudine and dolutegravir (ALD for short).
Speaking at the conference, Dr Leon Levin, a paediatrician who has been treating infants, children, and adolescents living with HIV for almost three decades, pointed out that the availability of new paediatric formulations had a major impact on the new treatment guidelines. (Spotlight previously reported on the registration of some of these new formulations here.) Levin is also the Senior Technical Advisor in Paediatrics at the NGO Right to Care.
One such child-friendly formulation is a 120/60mg scored, dispersible tablet of abacavir and lamivudine that can be taken in patients who weigh between 3 and 25kg. It is given once daily and two generics are registered with the South African Regulatory Authority (SAHPRA). “It’s going to literally replace all the other paediatric Abacavir+3TC formulations. You can swallow it, chew it, crush it, or dissolve it in water. So [it’s] very versatile,” he said.
Also important is a paediatric formulation of the antiretroviral dolutegravir – a medicine that forms the backbone of HIV treatment in adults. According to Levin, the child-friendly version of dolutegravir is not available to everyone yet, and many clinicians still need to undergo training on how to use it. It is a 10mg dispersible, scored tablet given once daily that can be used at 3kg and higher and from four weeks of age onward. There are two generic versions of this product registered with SAHPRA.
The introduction of paediatric dolutegravir is likely to overshadow the introduction of a four-in-one formulation of abacavir, lamivudine, lopinavir/ritonavir. The four-in-one combination has to be taken twice daily, is strawberry flavoured and comes in a powder form. “Unfortunately, this product to nobody’s fault was launched at the same time as paediatric dolutegravir. Which means paediatric dolutegravir is going to take centre stage and this product unfortunately is not going to be used much,” Levin said.
Updated guidelines
Levin explained that the changes to South Africa’s treatment guidelines focused on doing two main things when it comes to children living with HIV, the first is to implement an optimised regimen – the ALD regimen and the second is to create an “enabling environment to support engagement in care and adherence”. He said that with the new guidelines, we can expect “much improved [viral] suppression, optimised regimens, improved synchronisation of clinic visits, happier patients and their families and clinicians as well”.
A big change to the guidelines is that now children who weigh 3kg and are four weeks of age should be started on the ALD regimen, instead of the abacavir, lamivudine, and lopinavir/ritonavir regimen that was previously recommended. “This is a major change. It’s a fantastic, well-tolerated regimen. It’s potent and you’re going to get around a lot of the issues you had with these younger children,” Levin said.
Once the children on this regimen get to 30kg, they will be switched to a regimen containing tenofovir, dolutegravir, and lamivudine (TLD for short). TLD is also the regimen adults living with HIV in South Africa are offered when starting treatment for the first time.
For children who are already on treatment, the new guidelines recommend that all children who are four weeks of age and older and weigh 3kg or more should be transitioned to a dolutegravir-containing regimen. For children with suppressed viral loads, the switch to ALD or TLD is straightforward, while for children without viral suppression, it can get more complicated.
Another important change is that children over five years of age are now eligible for Repeat Prescription Collection Strategies (RPCs) if they are virally suppressed and had an age-appropriate disclosure, which means that their HIV status has been explained to them in a way that is appropriate for their age, as outlined in the guidelines. For children under five, they can be given a three months supply at a time, providing they are at least six months old. Levin pointed out that whenever RCPs or a three months supply is considered for children, it is essential to look at where and how the parents may be receiving their own antiretroviral treatment so that it can be co-ordinated, and parents don’t have to go to two different places to collect the medications.
New options in the pipeline
While the paediatric formulations included in the new guidelines are a step forward, there are experimental treatments in the pipeline that may make treatment yet more convenient for children.
“There’s a rich pipeline of new combinations and drug delivery developments. Hopefully, this will further improve access, clinical and virological outcomes,” Fairlie said in a conference presentation. “Obviously, the paediatric market is extremely small and then one has to maintain enthusiasm for manufacturers to actually continue to look at the paediatric population. And so, merging of treatments and prophylaxis regimens is really what would work going forwards.”
In her presentation, she specifically referred to long-acting formulations of cabotegravir (CAB-LA) and rilpivirine (RPV). CAB-LA has already been approved by SAHPRA for HIV prevention in adults and, as Spotlight reported last week, pilot projects evaluating how to best provide the CAB-LA injection in South Africa are set to start soon. The combination of CAB-LA and rilpivirine injections has been approved for the treatment of HIV in adults by the United States Food and Drug Administration, but not yet by SAHPRA. The injections are administered every two months.
Fairlie says that currently there are several studies either ongoing or set to start soon for the use of these agents in the paediatric and adolescent age groups. In addition, there are also trials planned to test another long-acting medication called lenacapavir in adolescents and broadly neutralising antibodies (bNAbs) in children.
She also highlighted several improved delivery methods that are in the pipeline for paediatrics. These include a mechanism that doesn’t require water, like oro-dispersible tablets, also known as fast melts, which disintegrate in the mouth as well as oral films that stick to the mouth, disintegrate there, and dissolve. There are also various tablet options that are small enough for children to swallow easily. Like multi-particulates, which are small and solid, multiple-unit dosages that can take the form of granules, pellets, or beads. Mini-tablets are also a prospect – these are compressed tablets no larger than 4ml. Finally, there are novel mechanisms like long-acting oral drug delivery systems and micro-array patches. Fairlie explained that long-acting oral drugs are where a drug is stored in the centre of a capsule that has a number of “arms”, which are able to keep the capsule in the stomach and slowly dissolve and release the drug into the stomach. This allows for slow-release dosing. The “arms” tend to break down after about seven days.
A study involving more than 745 000 adolescents from 41 countries across Europe and North America identified an increase in the amount of teenagers who underestimate their body weight. Tracking data from 2002 to 2018, the findings, published in Child and Adolescent Obesity, also show fewer adolescents overestimating their weight.
The team of international experts, who carried out the research, warn these shifting trends in body weight perception could reduce the effectiveness of public health interventions aimed at weight reduction in young people.
“During this impressionable age, body weight perception may influence a young person’s lifestyle choices, such as the amount and types of food they eat and their exercise habits,” says lead author Doctor Anouk Geraets, from the Department of Social Sciences, at the University of Luxembourg.
“So it’s concerning that we’re seeing a trend where fewer adolescents perceive themselves as being overweight — as this could undermine ongoing efforts to tackle increasing levels of obesity in this age group. Young people who underestimate their weight and therefore do not consider themselves to be overweight may not feel they need to lose excess weight and, as a result, they may make unhealthy lifestyle choices.”
A person’s perception of their body weight may not accurately reflect their actual weight. A discrepancy in body weight perception (BWP) may either be an underestimation (where actual weight is higher than perceived weight) or an overestimation (where actual weight is lower than perceived weight).
In the present study, the researchers examined survey data from 746,121 11-, 13- and 15-year-olds from 41 countries collected at four-yearly intervals between 2002 and 2018 in the International Health Behavior in School-Aged Children (HBSC), a WHO collaborative study.
The team modeled trends in BWP among adolescents across different countries over time, making adjustments for age, gender, and family socioeconomic status. They found:
Underestimation of weight status increased, and overestimation of weight status decreased over time among both sexes, with stronger trends for girls.
Correct weight perception increased over time among girls, while it decreased among boys.
Changes in correct weight perception, underestimation and overestimation of weight status differed across different countries — but these changes could not be explained by an increase in country-level overweight/obesity prevalence.
The authors speculated that the observed differences between girls and boys in BWP may support the idea there are sex differences in body ideals — and that these body ideals have changed over time. Notably, the increased underestimation and decreased overestimation of weight status over time for girls may be explained by the emergence of an athletic and strong body, as a new contemporary body ideal for both sexes.
“This study has clinical and public health implications. The increase in correct weight perception and the decrease in overestimation may have a positive effect on unnecessary and unhealthy weight loss behaviors among adolescents, while the increase in underestimation might indicate the need for interventions to strengthen correct weight perception,” says lead author Doctor Anouk Geraets.
“More research is now needed to understand the factors underlying these time trends and to develop effective public health interventions.”
While the large number of participating countries is a strength of the present study, but as these only included countries in Europe, the USA and Canada, the results can’t be generalised to other regions. In addition, although steps were taken to adjust the models for certain potential confounding factors, several other factors – such as body image, dieting, changing eating patterns, or migration – may also have played a role in the observed trends over time.
Research led by the University of Bristol has found that long COVID is not caused by an immune inflammatory reaction to COVID. Emerging data shows that immune activation may persist for months after contracting COVID. In this new study, published in eLife, researchers wanted to find out whether persistent immune activation and ongoing inflammation response could be the underlying cause of long COVID.
To investigate this, the Bristol team collected and analysed immune responses in blood samples from 63 patients hospitalised with mild, moderate or severe COVID at the start of the pandemic and before vaccines were available. The team then tested patients’ immune responses at three months and again at eight and 12 months post hospital admission. Of these patients, 79% (82%, 75%, and 86% of mild, moderate, and severe patients, respectively) reported at least one ongoing symptom with breathlessness and excessive fatigue being the most common.
Dr Laura Rivino, the study’s lead author, explained: “Long Covid occurs in one out of ten COVID cases, but we still don’t understand what causes it. Several theories proposed include whether it might be triggered by an inflammatory immune response towards the virus that is still persisting in our body, sending our immune system into overdrive or the reactivation of latent viruses such as human cytomegalovirus (CMV) and Epstein Barr virus (EBV).”
The team found patients’ immune responses at three months with severe symptoms displayed significant dysfunction in their T-cell profiles indicating that inflammation may persist for months even after they have recovered from the virus. Reassuringly, results showed that even in severe cases inflammation in these patients resolved in time. At 12 months, both the immune profiles and inflammatory levels of patients with severe disease were similar to those of mild and moderate patients.
Patients with severe COVID were found to display a higher number of long Covid symptoms compared to mild and moderate patients. However, further analysis by the team revealed no direct association between long COVID symptoms and immune inflammatory responses, for the markers that were measured, in any of the patients after adjusting for age, sex and disease severity.
Importantly, there was no rapid increase in immune cells targeting SARS-CoV-2 at three months, but T-cells targeting the persistent and dormant Cytomegalovirus (CMV) – a common virus that is usually harmless but can stay in your body for life once infected with it – did show an increase at low levels. This indicates that the prolonged T-cell activation observed at three months in severe patients may not be driven by SARS-CoV-2 but instead may be “bystander driven” ie driven by cytokines.
Dr Rivino added: “Our findings suggest that prolonged immune activation and Long COVID may correlate independently with severe COVID. Larger studies should be conducted looking at both a larger number of patients, including if possible vaccinated and non-vaccinated COVID patients, and measuring a larger range of markers and cytokines.
“Understanding whether inflammation and immune activation associate with Long COVID would allow us to understand whether targeting these factors may be a useful therapy for this debilitating condition.”
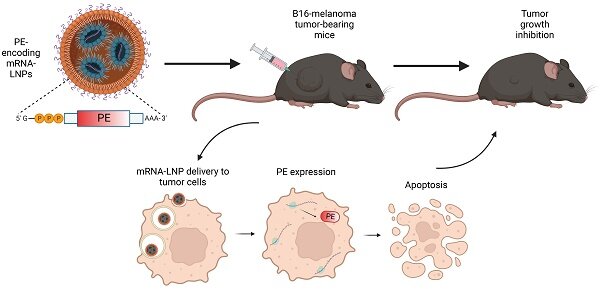
Tel Aviv University researchers have hit upon a novel method of cancer treatment by creating an mRNA ‘Trojan horse’ that instructed cancer cells to produce a toxin lethal to themselves, eventually killing them with a success rate of about 50%. This ground-breaking study was led by PhD student Yasmin Granot-Matok and Prof Dan Peer, a pioneer in the development of RNA therapeutics. The study’s results were published in Theranostics.
Prof Peer explains: “Many bacteria secrete toxins. The most famous of these is probably the botulinum toxin injected in Botox treatments. Another classic treatment technique is chemotherapy, involving the delivery of small molecules through the bloodstream to effectively kill cancer cells. However, chemotherapy has a major downside: it is not selective, and also kills healthy cells. Our idea was to deliver safe mRNA molecules encoded for a bacterial toxin directly to the cancer cells – inducing these cells to actually produce the toxic protein that would later kill them. It’s like placing a Trojan horse inside the cancer cell.”
First, the research team encoded the genetic info of the toxic protein produced by bacteria of the pseudomonas family into mRNA molecules (resembling the procedure in which genetic info of COVID-19’s ‘spike’ protein was encoded into mRNA molecules to create the vaccine). The mRNA molecules were then packaged in lipid nanoparticles developed in Prof Peer’s laboratory and coated with antibodies to ensure they would reach their target, the cancer cells. These particles were injected into the tumours of animal models with melanoma skin cancer. After a single injection, 44–60% of the cancer cells vanished.
“In our study, the cancer cell produced the toxic protein that eventually killed it,” says Prof Peer. “We used pseudomonas bacteria and the melanoma cancer, but this was only a matter of convenience. Many anaerobic bacteria, especially those that live in the ground, secrete toxins, and most of these toxins can probably be used with our method. This is our ‘recipe’, and we know how to deliver it directly to the target cells with our nanoparticles. When the cancer cell reads the ‘recipe’ at the other end it starts to produce the toxin as if it were the bacteria itself and this self-produced toxin eventually kills it. Thus, with a simple injection to the tumour bed, we can cause cancer cells to ‘commit suicide’, without damaging healthy cells. Moreover, cancer cells cannot develop resistance to our technology as often happens with chemotherapy – because we can always use a different natural toxin.”