Luc Montagnier, the French virologist credited as being a co-discoverer of the human immunodeficiency virus (HIV), has died aged 89. He jointly received the 2008 Nobel Prize was jointly awarded to Montagnier for his work in isolating the virus.
He was lauded for his crucial research, but in later life he was criticised for unscientific claims about autism and COVID.
Local news site FranceSoir reported that he died on Tuesday in Neuilly-sur-Seine “surrounded by his children”.
The virologist first began working on the virus in the early 1980s while at the Pasteur Institute in France. Montagnier and his team examined tissue samples from patients who had the mysterious new syndrome.
In 1983, Luc Montagnier’s team at the Pasteur Institute in Paris discovered HIV‑1. They cultured T cells from a lymph node biopsy from a 33-year-old homosexual French patient with symptoms that can precede AIDS (subsequently called pre-AIDS), such as lymphadenopathy. Finding that they had isolated a retrovirus, they were able to infect T cells from a healthy donor, but were unable to infect other cell types, including B cells and fibroblasts.
The group concluded that this patient at risk for AIDS was infected with a T cell–tropic retrovirus; however they could only tentatively associate it with AIDS. In 2008, Luc Montagnier and Françoise Barré-Sinoussi from his team were awarded the Nobel Prize for the isolation and characterisation of HIV-1.
However, US scientist Robert Gallo published similar findings in the same edition of Science in which the Pasteur team had announced theirs. He later concluded that the virus caused Aids. This led to years of heated debate over who actually discovered HIV.
Gallo revealed in 1991 that the virus he found came from the Pasteur Institute the year before, and the two men publicly agreed in 2002 that Montagnier’s team discovered HIV, but that Gallo first showed its role in causing Aids.
However, when Montagnier and Barré-Sinoussi were awarded the Nobel Prize in 2008 for their work – alongside Harald zur Hausen for his work on cervical cancer – the committee made no mention of Gallo, which provoked controversy.
Later on, Montagnier attracted great criticism for a series of unscientific claims, including over the causes of autism and later over the origins of COVID.
French media first reported that he had died at the American hospital in Neuilly-sur-Seine on 8 February, and his death was officially declared by authorities some time later.
Researchers have found, after reviewing a database containing 3 million pregnancies, that 1 in 16 women were exposed to teratogenic drugs.
The study, published in the American Journal of Obstetrics and Gynecology, highlights the need for women and their providers to carefully examine medications taken during pregnancy.
A teratogen is a substance that interferes with the normal development of a foetus. Hundreds of such drugs have been identified, including medications to treat seizures, migraines, obesity, acne, hypertension, bipolar disease and cancer.
University of Florida researchers investigated more than 200 teratogenic drugs and evaluated their exposure among 3.4 million pregnancies identified in a national private insurance database from 2006 to 2017. Prenatal exposure was defined by the mother taking at least one teratogenic drug during pregnancy.
The researchers divided drugs into two classes based upon their known teratogenic effect. About 140 drugs were known to have definite teratogenic effects, with another 65 identified as having potential teratogenic effects. The proportion of pregnancies with exposure to definite teratogens decreased slightly over the 12-year study period from 1.9% to 1.2%, while exposures for potential teratogens increased from 3.4% to 5.3%.
“While declining exposure rates among teratogenic drugs with definite risk are encouraging, the rising prenatal exposure to drugs with potential risk calls for more assessment,” study author Professor Almut Winterstein, PhD, RPh. “To have 1 in 16 women and their unborn baby exposed to a teratogenic medication is simply too high, and we must identify strategies to improve pregnancy outcomes.”
The study also examined age and risk for prenatal exposure to teratogenic drugs and found teenagers and women in their 40s had the greatest risk. Both groups are known to have more unintended pregnancies and the drug exposure may have been accidental, which points to the need for more information about effective birth control and family planning when using teratogenic drugs.
The researchers were especially interested in prenatal exposure during more recent years, following the enactment of FDA requirements for risk mitigation strategies. Those are designed to reinforce safe medication-use behaviors, such as a pregnancy test before a teratogenic drug is started, and only a few medications require this extra safety precaution.
The 12 drugs with mitigation protocols in the study were found to be used infrequently and contributed to only a small portion of prenatal exposures. More research and regulatory action are needed to optimise the use of medications during pregnancy, the researchers concluded.
“There is much to do to address the evidence available regarding the risk-benefit of many drugs during pregnancy, and the availability of adequate risk-mitigation programs that ensure pregnancies are not unnecessarily exposed to teratogenic drugs,” Prof Winterstein said. “In the meantime, women and their providers must rely on the written information that is provided about the teratogenic risk for drugs during pregnancy.”
The World Health Organization (WHO) has announced that the Eleventh Revision of the International Classification of Diseases (ICD-11) has now come into effect, with the latest update going online on Friday, 11th February.
Compared with previous versions, ICD-11 is entirely digital with a new user-friendly format and multilingual capabilities that reduce the chance of error. It has been compiled and updated with input from over 90 countries and unprecedented involvement of health-care providers, enabling evolution from a system imposed on clinicians into a truly enabling clinical classification and terminology database that serves a broad range of uses for recording and reporting statistics on health. It also allows entries to appear in multiple categories: for example, stroke appears under both the cardiovascular and neurological categories.
“International classification of diseases is the cornerstone of a robust health information system”, said Dr Samira Asma, the Assistant Director-General for Data, Analytics and Delivery for Impact at the World Health Organization (WHO). “ICD has been instrumental in helping us respond to the COVID pandemic using standardised data and continues to be crucial for tracking progress towards universal health coverage. We hope all countries will take advantage of ICD-11’s powerful new features.”
Among other updates, ICD-11 improves the clarity of terms for the general public and facilitates the coding of important details such as the spread of a cancer or the exact site and type of a fracture. The new version also includes updated diagnostic recommendations for mental health conditions and digital documentation of COVID certificates.
These updates reflect recent progress in medicine and advances in scientific understanding. For example, codes relating to antimicrobial resistance are now aligned with the Global Antimicrobial Resistance Surveillance System (GLASS). ICD-11 is also more capable of capturing data on health-care safety, thus identifying and reducing unnecessary events that may harm health such as unsafe workflows in hospitals.
ICD is used by health insurers who make reimbursement decisions on the basis of ICD coding, by national health programme managers, by data collection specialists, and by anyone who tracks progress in global health and determines health resource allocation.
“A key principle in this revision was to simplify the coding and provide users with all necessary electronic tooling – this will allow health-care professionals to more easily and completely record conditions,” says Dr Robert Jakob, Team Lead, Classifications Terminologies and Standards, WHO.
In addition to coding and capability updates, ICD-11 includes new chapters on traditional medicine, sexual health, and gaming disorder – which has now been added to the section on addictive disorders.
ICD-11 was adopted at the World Health Assembly in May 2019 and Member States committed to start using it for mortality and morbidity reporting in 2022. Since 2019, early adopter countries, translators, and scientific groups have recommended further refinements to produce the version that is posted online today.
A study may have found that a effects on a key gut bacteria are the reason why some patients experience diarrhoea after receiving the widely prescribed antibiotic amoxicillin-clavulanate.
Researchers, reporting in the journal iScience, found that the level of gut Ruminococcaceae, which plays a role in maintaining an individual’s gut health, strongly impacts diarrhoeal outcomes following antibiotic treatment.
One in three patients prescribed amoxicillin-clavulanate will develop diarrhoea. In some cases, it may be so severe that doctors have to prematurely halt the antibiotic, inadequately treating the infection or else forcing a change in antibiotics. The diarrhoea could also prolong patients’ hospital stays and further exposing them to hospital-acquired infections.
“The problem is very real for patients who are unable to take amoxicillin-clavulanate because it gives them diarrhoea, even though it is an effective and affordable antibiotic for their infection. Knowing why may help us identify those at risk of antibiotic-associated diarrhoea, and devise treatment strategies in the future to minimise or avoid such adverse effects,” said lead researcher Dr Shirin Kalimuddin.
The study recruited 30 healthy volunteers, each receiving a three-day oral course of amoxicillin-clavulanate. Their stool samples were collected over four weeks and analysed using gene sequencing to look for changes in the gut microbiome.
Ruminococcaceae levels in the stools of study volunteers who developed diarrhoea were significantly lower when compared to those who did not, both before and during treatment with amoxicillin-clavulanate. This suggests that individuals may, depending on their gut composition, be predisposed to antibiotic-associated diarrhea. The team further devised a simple polymerase chain reaction (PCR) test based on levels of Faecalibacterium prausnitzii, a species within the Ruminococcaceae family, that could potentially be used in clinical settings to quickly determine an individual’s risk of developing diarrhea with amoxicillin-clavulanate treatment.
“People respond differently to medication. Understanding this response and the ability to predict those at risk will help guide the development of point-of-care diagnostics,” said lead researcher Professor Eric J. Alm.
“While a lot of attention has been paid to how DNA influences a person’s response to medication, the impact of the gut microbiome on the human drug response has not been widely researched. Our findings provide evidence that an individual’s gut microbial composition can influence the risk of developing antibiotics-associated diarrhoea. Tested against amoxicillin-clavulanate, the study provides a framework to identify other potential causes of antibiotic-associated diarrhoea in relation to other classes of antibiotics,” added Prof Alm.
The next step would be a clinical trial to determine whether certain Ruminococcaceae could be used as a probiotic to prevent diarrhoea in patients prescribed antibiotics.
While the proposed National Health Insurance (NHI) could make use of existing private healthcare human resources, the necessary tax increases to fund it could drive more healthcare professionals from the country, the Professional Provident Society (PPS) has said. Economic and other factors, such as the Durban unrest, have already caused a surge of emigrations of professionals since July last year. In addition, foreign students graduates who study critical skills in South Africa (such as nurses and GPs) will no longer have an easy route to permanent residency.
The PPS, which counts about 30 000 healthcare professionals among its membership, pointed out the vulnerability of South Africa’s tax base – which has shrunk to only 6.9 million taxpayers, down from 7.6 million the year from the year before.
While it raised a number of concerns about the NHI, the group stated that it was broadly supportive of establishing universal healthcare in the country, and this goal could still be accomplished by using a dual public-private system. The PPS further noted that the government could benefit from the exceptional administrative capabilities and existing patient management systems.
However, NHI is dependent on strong, competitively remunerated human resources, with PPS pointing out that “South Africa has experienced a mass exodus of nurses in the 90s; we cannot risk that again. Both the government and private sector need to find a solution for South Africa and it cannot ‘import solutions’.”
“Professionals are a big proportion of healthcare delivery and the tax base. Their voices need to be considered.
“We urgently need to see the funding model, the implementation of the Health Market Inquiry (HMI) and details of how the system will work.”
The PPS said in a 2019 report that the highest risk to effective universal health cover in South Africa is losing highly skilled professionals to emigration. Healthcare professionals have a great deal of geographic freedom, and it is becoming easier to work in their trades the world over. COVID with its restrictions may have slowed emigrations by skilled professionals, but since July 2021, experts have seen a surge backed up by 18 months of pent-up demand.
The PPS noted that research has shown “that the decision to emigrate is a complex one that is driven by various personal and societal pull and push factors.” The NHI could be yet another push factor adding to the list of healthcare professionals’ sore points. “Healthcare worker migration from South Africa in the past has been driven by policy decisions and socio-economic and political considerations.
“In 2001, the number of nurse emigrants was roughly 20% of the total number working within the public sector in South Africa. That, together with being ranked as having the eighth-highest global number of emigrating physicians in the year 2000, created a dire situation for the sustainability of healthcare in South Africa at the time.”
Among general professionals, PPS’s research has indicated that many are considering emigration. A majority of respondents surveyed (73%) cited NHI as a potential reason for emigration, with 15% unsure and only 12% not considering leaving at all.
In addition to losses from emigration, the Department of Home Affairs has ended a 2014 waiver which allowed a quicker path to a residency permit for foreign students who acquire critical skills in South African higher learning institutions. Going forward, foreign students will no longer be able to apply for permanent residency visas without complying with the usual requirements such as providing proof of five years’ work experience. This is seen as detrimental to South Africa’s ability to attract and retain skilled professionals. This may further impact NHI implementation as the necessary skilled human resources are squeezed further as fewer foreign students may choose to study and then work in South Africa.
In a study published in Arthritis & Rheumatology, people with hand osteoarthritis, higher body mass index was associated with greater pain severity in the hands, feet, knees, and hips.
Osteoarthritis is one of the most debilitating joint disorders worldwide, affecting up to 10% of men and 13% of women. Osteoarthritis is characterised by a progressive onset of joint damage, commonly associated with pain. Joints commonly affected include the knee, hip and hand. Various stressors, risk factors and genetics may predispose an individual to developing osteoarthritis in a particular joint.
In a study of 281 patients, researchers noted that observed associations of body mass index with hand pain and total body joint pain seemed to involve certain inflammatory markers (leptin and high-sensitivity C-reactive protein, respectively).
The researchers suggest that systemic effects of obesity, measured by leptin, could have a larger mediating role for pain in hands than in lower extremities. Low-grade inflammation, measured by hs-CRP, may contribute to generalised pain in overweight or obese individuals.
“Our results highlight the complexity of pain in hand osteoarthritis. Obesity is not only leading to pain through increased loading of joints in the lower extremities, but seems to have systemic effects leading to pain in the hands and overall body,” said lead author Marthe Gløersen, MD, of Diakonhjemmet Hospital, in Norway.
By sequencing genes linked to cardiac arrhythmia risk in more than 20 000 people without an indication for genetic testing, scientists were able to identify possible pathogenic variants in 0.6% of individuals, according to a study published in Circulation.
This rate is higher than those previously reported, according to Carlos G. Vanoye, PhD, research associate professor of Pharmacology and a co-author of the study.
“This study suggests the prevalence of genetic susceptibility to cardiac arrhythmia may be underestimated,” Dr Vanoye said.
The American College of Genetics and Genomics (ACMG) currently recommends that incidentally discovered pathogenic or likely pathogenic variants in 73 Mendelian disease genes be reported back to patients. This includes many genetic variants associated with congenital cardiac arrhythmias, causing irregular heartbeats which can lead to stroke or sudden cardiac death.
However, the pathogenicity of many genetic variants in these known arrhythmia genes is uncertain, and classification of these variants is still in the early stages.
“A person can carry a disease-causing gene variant but exhibit no obvious signs or symptoms of the disease,” Dr Vanoye said. “Because the genes we studied are associated with sudden death, which may have no warning signs, discovery of a potentially life-threatening arrhythmia gene variant can prompt additional clinical work-up to determine risks and guide preventive therapies.”
The current study used data from the Electronic Medical Records and Genomics sequencing (eMERGEIII) study. The eMERGEIII study investigated the feasibility of population genomic screening by sequencing 109 genes implicated across the spectrum of Mendelian (single inherited gene mutation) diseases in over 20 000 individuals, returning variant results to the participants, and using Electronic Health Record (EHR) and follow-up clinical data to ascertain patient phenotypes.
In the current study, investigators analysed 10 arrhythmia-associated genes in individuals without an indication for genetic testing.
The researchers determined the functional consequences of these variants of uncertain significance and used the data to refine the assessment of pathogenicity. In the end, they reclassified 11 of these variants: three that were likely benign and eight that were likely pathogenic.
In all, 0.6% of the studied population had a variant that increases risk for potentially life-threatening arrhythmia and there was overrepresentation of arrhythmia phenotypes among these patients. This is a rate higher than previously known for genetic arrhythmia syndromes (approximately 1 in 2000) and illustrates the potential for population genomic screening, Dr Vanoye said.
“Population genomic screening can positively affect public health. Many rare, disease-associated variants can be found this way which can then help determine the disease-risk of the carriers of these variants,” Dr Vanoye said. “Although the costs of genomic screening may be currently high, assessing patient risk followed up by clinical care would reduce the financial and emotional cost of the disease.”
Almost a third of older adults infected with COVID in 2020 developed at least one new condition requiring medical attention in the months after initial infection, compared to only a fifth who were not infected, according to a study published by The BMJ.
Conditions involved a range of major organs and systems, including the heart, kidneys, lungs and liver as well as mental health complications. Some studies now examine the frequency and severity of sequelae after COVID infection, but few have described the excess risk of new conditions triggered by COVID infection in adults 65 and older.
Researchers used US health insurance records to identify 133 366 individuals aged 65 or older in 2020 who were diagnosed with COVID before 1 April 2020. Three (non-COVID) comparison groups were matched: from 2020, 2019, and a group diagnosed with viral lower respiratory tract illness.
The researchers then recorded any persistent or new conditions starting 21 days after a COVID diagnosis (the post-acute period) and calculated the excess risk for conditions triggered by COVID over several months based on age, race, sex, and whether patients were hospitalised with COVID.
The results show that among individuals diagnosed with COVID9 in 2020, 32% sought medical attention in the post-acute period for one or more new or persistent conditions, which was 11% higher than the 2020 comparison group.
Compared with the 2020 comparison group, COVID patients were at increased risk of developing a range of conditions including respiratory failure (an extra 7.55 per 100 people), fatigue (+5.66 per 100), high blood pressure (+4.43 per 100), and mental health diagnoses (+2.5 per 100). Similar findings were found for the 2019 comparison group.
However, compared with the group with viral lower respiratory tract illness, only respiratory failure, dementia, and fatigue showed increased risk differences of 2.39, 0.71, and 0.18 per 100 people with COVID, respectively.
Individuals hospitalised with COVID had a markedly increased risk for nearly all conditions. The risk of several conditions was also increased for men, for those of black race, and for those aged 75 and older.
Limitations include being an observational study – however, the authors warn that the number survivors with sequelae will continue to grow.
“These findings further highlight the wide range of important sequelae after acute infection with the SARS-CoV-2 virus,” they write. “Understanding the magnitude of risk for the most important clinical sequelae might enhance their diagnosis and the management of individuals with sequelae after acute SARS-CoV-2 infection.”
“Also, our results can help providers and other key stakeholders anticipate the scale of future health complications and improve planning for the use of healthcare resources,” they conclude.
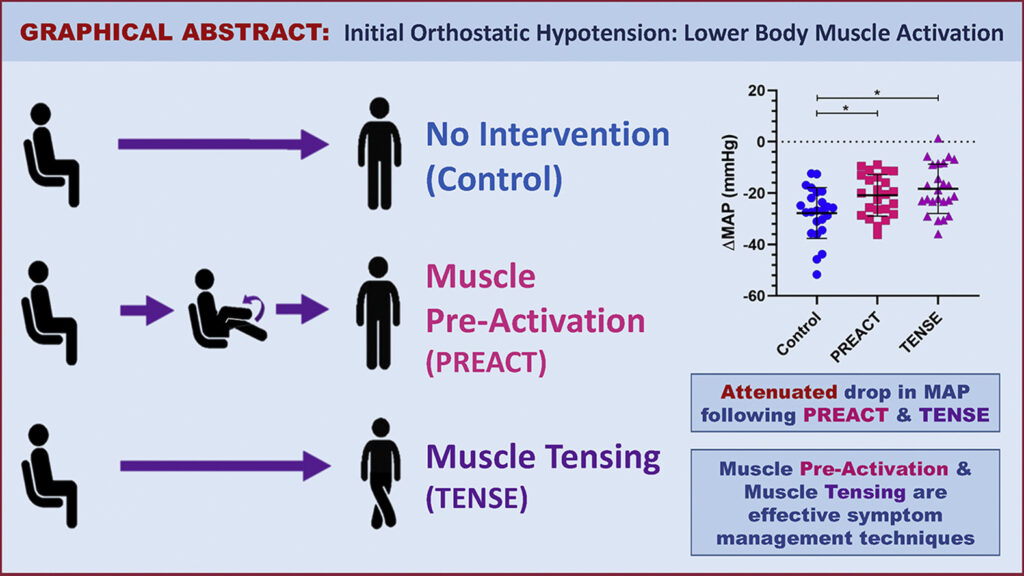
Light-headedness upon standing up due to initial orthostatic hypotension (IOH) is a common but poorly understood condition. A new study offers two simple techniques to effectively manage symptoms of IOH and improve quality of life by activating lower body muscle before or after standing. The research appears in Heart Rhythm.
IOH is a transient decrease in blood pressure and increase in heart rate. Syncope, light-headedness, dizziness, or loss of consciousness from IOH, affects up to 40% of the general population (all ages), while presyncope is probably even more common. However, the condition is under-studied and there are very few options currently available to patients with IOH and no pharmacological treatments. The most common recommendations have been to stand up slowly or sit up first before standing.
IOH symptoms often present during an active stand but not with a passive tilt-table test, suggesting that a muscle activation response plays an important role in the pathophysiology of IOH. This muscle activation response refers to the rapid and excessive vasodilation that occurs in response to the brief lower body muscle contraction required to stand due to local mechanisms. Additional factors involved in this response include the increase in heart rate, initially due to the muscle heart reflex and secondarily in response to the arterial baroreflex triggered by the drop in BP as well as the increase in peripheral resistance, which is also triggered by the arterial baroreflex.
This study investigated physical manoeuvres before or after standing and their efficacy in reducing the drop in blood pressure as well as the symptoms typically seen in IOH patients upon standing. Study participants included 24 young women with a history of IOH. Two participants had inadequate heart rate recordings and were excluded from the analysis. The interventions tested consisted of lower body muscle pre-activation (thighs) through repeated knee raises prior to standing (PREACT) and lower body muscle tensing (thighs and buttocks) through leg crossing and tensing immediately after standing (TENSE).
The 22 study participants completed three sit-to-stand manoeuvres including a stand with no intervention (control), and two interventions. Researchers found that both PREACT and TENSE effectively improve the blood pressure drop. This led to a reduction in symptoms upon standing. They found that the PREACT manoeuvre accomplished this by increasing cardiac output, while the TENSE manoeuvre did so by increasing stroke volume.
“Our study provides a novel and cost-free symptom management technique that patients with IOH can use to manage their symptoms,” noted first author Nasia A. Sheikh, MSc. “Since it is a physical manoeuvre, it simply requires the lower body limbs, which patients can utilise at any time and from anywhere to combat their symptoms.”
A clot within a blood vessel interrupting blood flow to the brain. Copyright American Heart Association
Ischaemic stroke patients previously considered unlikely to survive without severe disability may regain far more function if the blood clots are mechanically removed in addition to standard medical therapy, according to preliminary late-breaking research presented today at the American Stroke Association’s International Stroke Conference 2022.
In 2018, the American Heart Association’s stroke treatment guidelines were updated to recommend endovascular therapy (mechanical clot removal) for select stroke patients to improve the odds of functional recovery. This new study in Japan is the first randomised, controlled trial to demonstrate the effectiveness of endovascular therapy in patients with severe strokes involving clots in one or more large brain arteries, causing a large blood flow interruption in the brain. This approach had worked for patients with fewer areas of the brain disrupted, however, clinical experience was mixed for patients with more severe strokes.
Infarction area, or core area, estimates the volume of brain affected and describes the blockage location as seen on a brain CT. A lower number translates to a stroke affecting more core areas of the brain: 8-10=small core, 6-7=moderate core and 0-5=large core. Current US stroke guidelines recommend endovascular therapy for core areas 6-9. This study examined blockages that scored as 3-5. Strokes with blockages measuring 0-2 core areas are considered too severe and highly unlikely the patient would return to ambulatory independence.
“I have often encountered a dramatic improvement in a patient just after the mechanical clot removal procedure, even when the infarction area was large. Yet, patients sometimes also experienced severe haemorrhagic transformation [a life-threatening complication that occurs when blood from outside the brain crosses the blood-brain barrier and worsens stroke outcome] after the artery was reopened. So, in Japan, our stroke physicians are always cautious about endovascular therapy when the infarction area is large,” said Professor Shinichi Yoshimura, lead author of the study.
This randomised study included 203 stroke patients (average age of 76 years; 44% women). Most (71%) were examined and had MRI or a CT scan of the brain within 6 hours after stroke symptoms were first noticed, when patients are generally considered eligible for endovascular therapy. The other patients were seen between 6-24 hours after symptoms were noticed, and additional imaging showed areas of the brain that might benefit from prompt treatment.
On imaging, all patients were found to have clots blocking a large cerebral artery – either the internal carotid artery, the proximal middle cerebral artery or both. The strokes were rated as severe (median 22 on the National Institutes of Health (NIH) Stroke Scale,) and involved disrupted blood flow to large areas of the brain (about 7 out of 10 regions).
After imaging, the patients were randomly selected to receive either standard medical care for stroke (intravenous fluids, controlling blood pressure and other risk factors, and thrombolytics for lower bleeding risk patients) or standard medical care plus endovascular therapy performed within an hour after imaging to mechanically remove the clots. Due to bleeding concerns, intravenous thrombolytics were sparingly administered to select patients in a similar proportion in both treatment groups (27 of those who received endovascular therapy and 29 who received standard care).
Comparing the 100 patients who received endovascular therapy with 102 on standard therapy alone, the analysis found:
Patients who received endovascular therapy were 2.43 times more likely (31% vs 13%) to be able to walk unassisted and to have a residual disability rated as none to moderate 90 days later.
After 90 days, more of the patients (14% vs. 6.9%) who received endovascular therapy were considered functionally independent, meaning they were either able to carry out all their pre-stroke activities or to have a slight disability that did not require daily assistance.
At 48 hours after treatment, more of the patients (31% vs. 8.8%) who received endovascular therapy had major early neurological improvement.
“Our findings confirm that anyone who suffers from stroke should be transferred to a medical facility capable of endovascular therapy as soon as possible. The benefit of endovascular therapy is not limited by the severity or region of a stroke. These patients may have the chance to more fully recover from stroke and go back to their previous lives and activity levels,” said Professor Takeshi Morimoto, senior author of the study.
Several outcomes were compared to evaluate the safety of adding endovascular therapy to medical treatment, with researchers reporting:
Within 48 hours, scans revealed that more of the patients who received endovascular therapy had experienced some bleeding within the brain (with or without symptoms), 58% vs. 31%, respectively.
However, the number of patients who experienced other adverse outcomes was similar in the two treatment groups. The adverse events included brain bleeding within 48 hours that caused a worsening of neurological status (4 points or greater worsening on the NIH Stroke Scale); the need for surgery to relieve pressure on the brain in the first week; death within 90 days; or the recurrence of ischaemic stroke within 90 days.
“The finding of more intracranial bleeding in the patients who received endovascular therapy is very important. However, there were haemorrhages with symptoms and some that caused no symptoms. The haemorrhages with no symptoms were detected on imaging conducted for this study in the endovascular treatment group, not in the standard practice group. Symptomatic intracranial haemorrhage still occurred more commonly among patients in the endovascular group, however, it was not a statistically significant difference from the standard care group,” Morimoto said.
Due to different treatment protocols in Japan, where there is less use of intravenous thrombolysis than in the US and other western countries, and where more strokes are imaged with MRI than CT, this study’s results may over- or underestimate the effectiveness of endovascular therapy.
The researchers are currently performing sub-analyses to help identify factors that might signal which patients are more likely to have a greater return of function after the treatment. “In addition, tools, devices or rehabilitation methods that could potentially improve the likelihood for similar patients to recover with less disability should be investigated,” Morimoto said.