University of Southampton researchers have found that the link between smoking at the start of pregnancy and having a smaller baby may extend to future pregnancies.
The research team studied data between 2003 and 2018 for nearly 17 000 mothers who received antenatal care for their first two pregnancies.
The findings, published in PLOS One, showed that, compared to non-smokers, women who smoked at the start of their first pregnancy were more likely to have a baby born smaller than expected in their second pregnancy. This held true even where they quit by the start of their second pregnancy.
The link between smoking during a pregnancy and that baby’s birth weight is well established. However, until now there has been limited evidence on the impact of maternal smoking on following pregnancies.
This study found that for women who smoked but did not smoke at the start of either pregnancy, there was no extra risk of a small for gestational age (SGA) baby in the second pregnancy compared to non-smokers. A mother who smoked ten or more cigarettes a day at the start of both of her first two pregnancies had the highest odds of SGA birth.
Study leader Dr Nisreen Alwan, Associate Professor at the University of Southampton, said: “It is important to encourage women to quit smoking before pregnancy and to not resume smoking after the baby is born. Resources that support mothers to quit and maintain smoking cessation are needed.”
First author Elizabeth Taylor said: “Women who smoke between pregnancies can reduce the risk of having a SGA baby by stopping smoking before the start of their next pregnancy. The period between pregnancies is when most mothers have close contact with health and care professionals and may require support to stop smoking.”
It is hoped that these findings and future research will encourage healthcare professionals and commissioners to provide better support to women before and between pregnancies, helping them to quit smoking, leading to better health for both mothers and children.
Saliva samples are easy to obtain and useful for measuring antibodies to SARS-CoV-2 in children, which could improve epidemiological surveillance in school settings. The study followed over 1500 children who went to summer schools in Barcelona last year. The results were published in BMC Medicine.
One of the pressing questions during this pandemic has been to understand children’s susceptibility to SARS-CoV-2 infection and how they infect others. An obstacle to answer this question is that most infections in children are mild or asymptomatic, and are therefore missed. To establish whether an individual has been exposed to SARS-CoV-2 in the past, virus-specific antibodies in blood need to be detected. Measuring antibody prevalence over time in a cohort of children can provide very valuable epidemiological information. However, this requires techniques that are both sensitive and minimally invasive.
In this study, performed through the Kids Corona platform, the team led by Carlota Dobaño, from the Barcelona Institute for Global Health (ISGlobal), and Iolanda Jordan, from Hospital Sant Joan de Déu (HSJD), used saliva instead of blood to measure virus-specific antibodies in over 1500 children who attended different summer schools in Barcelona in 2020, as well as around 400 adult staff. Two saliva samples per participant were analysed, one at the beginning and one at the end of the camp stay, and different antibody types (IgG, IgA and IgM) targeting different viral antigens were measured.
The study found that 3.2% of the participants developed antibodies between the first and second sample, indicating new infections. This is six times higher than the infection rate estimated by weekly PCR screening. “It has been reported that some children can be positive for antibodies despite being negative by PCR, which suggests that they can generate an immune response that prevents the establishment of SARS-CoV-2 infection,” explained Dobaño, first author of the study. It could also be because asymptomatic children have lower viral loads or that their viral clearance is faster.
Furthermore, the analysis shows that the percentage of new infections was higher in adults (2.94%) than in children (1.3%), suggesting differences in infection and transmission dynamics. Finally, contrary to blood tests, asymptomatic people had higher levels of anti-Spike antibodies in saliva, suggesting these antibodies play a protective role in respiratory mucosae. “This means that anti-Spike antibodies in saliva could be used to measure protective immunity upon vaccination, especially in the case of intranasal vaccines,” said senior study co-author Gemma Moncunill.
“We previously demonstrated in other Kids Corona studies that saliva is useful for detecting virus by PCR. With this study, we demonstrate that it’s also an effective and much friendlier way to measure antibodies, making it the ideal sample for children, instead of the more invasive nasal swab,” said Jordan.
Older women are more likely to struggle with both regular daily tasks and mobility activities, according to new analysis of longitudinal cohort studies.
However, the researchers say disparities in ability to perform daily tasks have been steadily decreasing as the socioeconomic gap between the sexes has decreased.
The international study, published in The Lancet Healthy Longevity, uses data from more than 27 000 men and 34 000 women aged 50 to 100, born between 1895 and 1960, to examine sex differences in daily activity and mobility limitations. Researchers at UCL and the National Institute of Health and Medical Research (INSERM) in France drew on four large longitudinal studies, covering 14 countries*.
Women were more found to be more likely than men to be limited in their ‘functional capacity’ (both tasks and mobility) as they get older. From age 75, women were also more likely to have three or more mobility issues (such as going up a flight of stairs) or limitations with more complex daily tasks (eg managing money) compared to men who were more likely to have just one or two. At age 85 years, the prevalence of three or more mobility limitations was 10% higher in women than in men.
Lead author, Mikaela Bloomberg, UCL PhD candidate, explained: “Our study of over 60,000 participants born between 1895 and 1960 provides new insights on functional limitations and sex differences.
“We found that women are more likely to be limited than men in carrying out daily tasks from age 70, while we observed women were more likely to be limited in mobility activities from age 50 onward.
“This is an important observation because mobility limitations can precede other more severe limitations and targeting these gaps at middle age could be one way to reduce sex differences in limitations at older ages.”
Historical socioeconomic differences between men and women in areas such as education and entrance to the labour force may partly explain these differences, as women are disproportionately exposed to associated health risks that can lead to disability.
“It appears that gender inequalities in the ability to carry out daily tasks at older age are decreasing over time and this could be explained by the fact that women have better access to education and are more likely to enter the paid labour force in recent generations,” said Bloomberg.
“And although reductions in socioeconomic inequalities may be associated with smaller disparities in simple daily tasks, we did not see the same reductions in sex disparities for mobility after accounting for socioeconomic factors. This might be partly due to sex differences in body composition such as body mass and skeletal muscle index but more research is needed to identify other factors.”
Co-author Dr Séverine Sabia added: “Developing targeted prevention policies to preserve independent living and quality of life for older adults requires an understanding of drivers of sex differences in functional limitations.
“Our study indicates improvements in socioeconomic conditions for women could play an important role in reducing these sex differences. Findings also highlight the importance of early prevention to tackle sex differences in mobility that may trigger sex differences in disability at older age.”
Researchers examining the development of resistance to HIV drugs have uncovered a mechanism of drug resistance development in combination therapy, where ‘windows’ open up for resistance to develop.
In the late 1980s, when HIV treatments were first introduced, patients would often develop resistance to those treatments within six months. The introduction of triple-drug treatment regimens in the 1990s was intended to rectify that. Even if the virus developed resistance to one drug, two others would still knock it out – in theory. Unfortunately, some patients still develop resistance, leaving scientists with a critical question to answer: Why?
“There’s all these things that we still don’t understand, like why do we even get resistance when treating with three drugs,” said San Francisco State University Associate Professor of Biology Pleuni Pennings. “We understand why it is becoming less common, but it should have been zero all along.”
Prof Pennings and her colleagues offer explanations for this phenomenon in a study published in eLife.
Several interesting observations were noted from analysis of HIV patient records. Drug resistance can evolve years after successful therapy, often the result of sequential mutations that occur in a predictable order. Current models could not explain these observations, and while some studies identify mutations that confer drug resistance, they don’t address how and where they arise.
Drawing on two computational models, the researchers suggest that these observations may result from drug heterogeneity over time and throughout the body. While patients receive three HIV therapies simultaneously, drugs have different half-lives and patients do not always adhere to therapy regimens. This could create opportunities for drug resistance evolution, during a window when only one drug is active. Drugs also don’t uniformly penetrate the entire body, meaning that in some locations in a patient’s body, only one of the drugs might be active, creating another evolution and escape opportunity.
“I think one main reason why we should care is actually not because of HIV but because of drug resistance in other situations,” Prof Pennings explained.
Although drug resistance among patients with HIV is fairly low, drug resistance to multidrug therapies is a big problem for diseases such as malaria and tuberculosis. In addition, the COVID pandemic and the rise of variants show how our understanding of evolving pathogens is still lacking.
“In a way, HIV is the poster child of how we solved drug resistance. … [But] if we don’t understand how we did it, then it’s really hard to take these lessons to other situations,” Prof Pennings said.
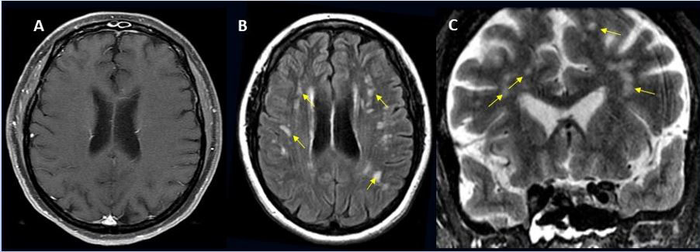
49-year-old female with past medical history of mitral valve disease and tricuspid valve regurgitation who developed headache followed by cough and fever presented to the ER with right upper eyelid ptosis (drooping). Credit: Radiological Society of North America and Scott H. Faro, M.D.
Approximately one in 100 patients hospitalised with COVID will likely develop complications of the central nervous system, according to a large international study. These can include stroke, haemorrhage, and other potentially fatal complications. The study was presented at the annual meeting of the Radiological Society of North America (RSNA).
“Much has been written about the overall pulmonary problems related to COVID, but we do not often talk about the other organs that can be affected,” said study lead author Scott H. Faro, MD, FASFNR, professor of radiology and neurology at Thomas Jefferson University. “Our study shows that central nervous system complications represent a significant cause of morbidity and mortality in this devastating pandemic.”
Dr Faro initiated the study after finding that only a small number of cases informed existing literature on central nervous system complications in hospitalised COVID patients.
To build a more complete picture, he and his colleagues analysed nearly 40 000 cases of hospitalised COVID patients, admitted between September 2019 and June 2020. Their average age was 66 years old, and two thirds were men.
Confusion and altered mental status were the most common causes of admission followed by fever. Comorbidities such as hypertension, cardiac disease and diabetes were common.
There were 442 acute neuroimaging findings most likely associated with the viral infection, with central nervous system complications in 1.2% of this large patient group.
“Of all the inpatients who had imaging such as MRI or a CT scan of the brain, the exam was positive approximately 10% of the time,” Dr Faro said. “The incidence of 1.2% means that a little more than one in 100 patients admitted to the hospital with COVID are going to have a brain problem of some sort.”
Ischaemic stroke, with an incidence of 6.2%, was the most common complication, followed by intracranial haemorrhage (3.72%) and encephalitis (0.47%).
A small percentage of unusual findings was uncovered, such as acute disseminating encephalomyelitis, an inflammation of the brain and spinal cord, and posterior reversible encephalopathy syndrome, a syndrome that mimics many of the symptoms of a stroke.
“It is important to know an accurate incidence of all the major central nervous system complications,” Dr Faro said. “There should probably be a low threshold to order brain imaging for patients with COVID.”
The emergence of the Omicron SARS-CoV-2 variant which has resulted in renewed lockdowns and travel bans around the world, which have been criticised by the WHO. In contrast, South Africa will stick to an adjusted Level 1 lockdown for the time being, though pushing for mandatory vaccinations. Business and civil society groups had warned that increasing restrictions would have provoked backlash as recent election campaign events had effectively ignored them.
Many nations around the world have reacted quickly to the new variant, which has a large number of mutations compared to the Delta variant. The UK’s decision to suspend flights from South Africa as well as nine other African countries has provoked criticism from a number of quarters, including President Cyril Ramaphosa. The sudden move has caught many travellers by surprise, including a Welsh rugby team which had two members test positive, one of which was for Omicron. They will have to self-isolate before they are able to return, depending on flight availability.
Japan and Israel have taken the more extreme steps of closing their borders to foreigners. The first cases of Omicron that were recorded in Botswana were revealed to be in visiting diplomats, although which country they came from has not been revealed.
The World Health Organization criticised the imposition of travel restrictions, acknowledging that although they may play a role in slightly reducing the spread of COVID, they still place a heavy burden on lives and livelihoods. It pointed out that if restrictions are implemented, they should not be unnecessarily invasive or intrusive, and should be scientifically based, under international law, the International Health Regulations. It notes South Africa followed International Health Regulations, and informed WHO as soon as its national laboratory identified the Omicron variant.
“The speed and transparency of the South African and Botswana governments in informing the world of the new variant is to be commended. WHO stands with African countries which had the courage to boldly share life-saving public health information, helping protect the world against the spread of COVID,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “On the eve of a special session on pandemic preparedness I urge all countries to respect their legal obligations and implement scientifically based public health actions. It is critical that countries which are open with their data are supported as this is the only way to ensure we receive important data in a timely manner.”
Although a full picture of the new variant’s severity is still two or three weeks away, Angelique Coetzee, chair of the South African Medical Association, told the AFP she had recently seen around 30 patients at her Pretoria practice who tested positive for COVID but had unfamiliar symptoms.
“What brought them to the surgery was this extreme tiredness,” she said, something she said was unusual for younger patients. Most were men under 40, and just under half were vaccinated. Other symptoms included mild muscle aches, a “scratchy throat” and dry cough, she said. Just a few had a slightly high temperature. These very mild symptoms stand in contrast to other variants, which typically result in more severe symptoms.
Viral RNA levels in the blood is a reliable indicator in predicting COVID mortality, according to a study published in Science Advances.
“In our study, we were able to determine which biomarkers are predictors of mortality in the 60 days following the onset of symptoms,” said Université de Montréal medical professor Dr. Daniel Kaufmann, the study’s co-lead author alongside colleagues Nicolas Chomont and Andrés Finzi.
“Thanks to our data, we have successfully developed and validated a statistical model based on one blood biomarker,” viral RNA, Prof Kaufmann said.
Despite advances in COVID management, identifying patients at greater risk of dying of the disease has been difficult. Other studies identified various biomarkers, but assessing so many parameters is not possible in a clinical setting and gets in the way of doctors’ quick clinical decision-making ability.
Using blood samples from 279 patients hospitalised for COVID of differing severity, Kaufmann’s team measured amounts of inflammatory proteins, looking for any that stood out.
At the same time, Chomont’s team measured the amounts of viral RNA and in Finzi’s the levels of antibodies targeting the virus. Samples were collected 11 days after the onset of symptoms and patients were monitored for a minimum of 60 days after that.
The goal: to test the hypothesis that immunological indicators were associated with increased mortality.
“Among all of the biomarkers we evaluated, we showed that the amount of viral RNA in the blood was directly associated with mortality and provided the best predictive response, once our model was adjusted for the age and sex of the patient,” said Elsa Brunet-Ratnasingham, a doctoral student in Kaufmann’s lab and co-first author of the study.
“We even found that including additional biomarkers did not improve predictive quality,” she added.
Prof Kaufmann and Brunet-Ratnasingham tested the model on two independent cohorts of infected patients from Montreal’s Jewish General Hospital (recruited during the first wave of the pandemic) and the CHUM (recruited during the second and third waves).
No matter which hospital the patients were treated at, nor which period of the pandemic they fell into: in all cases, the predictive model worked. Now Prof Kaufmann and his colleagues want to put it to practical use.
“It would be interesting to use the model to monitor patients,” he said, “with the following question in mind: when you administer new treatments that have proven effective, is viral load still a predictive marker of mortality?”
A new study has shown that a clutter-free environment may not help people living with dementia carry out daily tasks.
Researchers studied whether people with dementia were better able to carry out tasks, such as making a cup of tea, at home amidst their normal clutter or in a clutter-free environment. Surprisingly, participants with moderate dementia performed better when surrounded by their usual clutter. But the different environments made no difference to people with mild and severe dementia, who were able to perform at the same level in both settings. The findings were published in Alzheimer Disease & Associated Disorders.
Prof Eneida Mioshi, from the University of East Anglia. said: “As dementia progresses, people gradually lose their ability to carry out daily tasks due to changes in their cognitive, perceptual and physical abilities. Participation in daily tasks could then be improved by adapting the person’s environment.
“To this end, we wanted to investigate the role of clutter in activity participation, given the potential to use de-cluttering to support people with dementia to continue to be independent.
“Environmental clutter has been defined as the presence of an excessive number of objects on a surface or the presence of items that are not required for a task. It is generally assumed that a person with dementia will be better-able to carry out daily tasks when their home space is tidy and clutter free. However there has been very little research to really test this hypothesis.
“We wanted to see whether clutter was negatively affecting people with dementia. So we studied how people at different stages of dementia coped with carrying out daily tasks at home, surrounded by their usual clutter, compared to in a clutter-free setting – a specially designed home research lab.”
Occupational therapist and PhD student Julieta Camino carried out the study with 65 participants. They were grouped into those with mild, moderate and severe dementia, and were asked to carry out daily tasks including making a cup of tea and making a simple meal, both at their own home and at UEA’s specially designed NEAT research bungalow, a fully furnished research facility that feels just like a domestic bungalow.
The researchers evaluated performance of activities in both settings, and also measured the amount of clutter in the participants’ homes. Meanwhile the NEAT home setting was completely clutter free.
A new study in the US has found that complications from extreme heat appear to be more pronounced among young and middle-aged adults than older adults.
Extreme heat poses an increasing threat to the public, due to the continued effects of climate change. Although the adverse health impacts of heat have been well documented among older adults, less is known about the potential impacts of heat on young and middle-aged adults.
Published in the BMJ, the study examined the relationship between extreme temperatures and emergency department (ED) visits, and found that days of extreme heat were associated with an increase risk of ED visits for any cause, heat-related illness, renal disease, and mental disorders among all adults, but the strongest association was found among adults ages 18-64.
Prior research on heat’s health impacts have mostly focused on mortality or hospital admissions among seniors. This study is the first national-scale assessment of extreme heat effects on adults of all ages, measured with ED visits.
“Many illnesses that lead to utilisation of the ED do not lead to hospitalisation because they can be treated in a short amount of time, particularly among the younger adult population,” said study senior author Gregory Wellenius, professor of environmental health and director of the Program on Climate and Health at SPH. “By looking at emergency room visits, we aimed to obtain a more comprehensive picture of the true burden of disease that might be attributed to the days of high heat.”
Prof Wellenius and colleagues analysed healthcare claims data to quantify the risk of ED visits for any cause and for heat-associated conditions during the warm season (between May and September) from 2010 to 2019.
For the study, the researchers analysed claims data among 74 million adults, including more than 22 million ED visits. They found that days of extreme heat (varying by location, but averaging about 34°C), were associated with a 66% greater risk of ED visits for heat-related illness, as well as a 30% increased risk for renal disease, compared to ED visits on cooler days. But the risk according to extreme heat varied by age. A day of extreme heat was associated with a 10.3% higher risk of ED visits among people ages 45 to 54 years old, compared to a 3.6% higher risk among those older than 75.
“Younger adults may be at greater risk of exposure to extreme heat, particularly among workers that spend substantial time outdoors,” says study lead author Shengzhi Sun, research scientist in the Department of Environmental Health at SPH. “Younger adults may also not realise that they too can be at risk on days of extreme heat.”
Prior studies had shown that people in US counties with lower warm-season temperatures still experience higher risks of heat-related complications. “While extreme heat threatens everyone’s health, this study provides further evidence that it is especially dangerous in regions with cooler climates that may be less adapted to heat,” says study co-author Kate Weinberger, assistant professor at the University of British Columbia’s School of Population and Public Health. “As temperatures continue to rise due to climate change, the implementation of heat adaptation measures in these regions will be critically important.”
According to the researchers, many of these heat-related complications can be prevented through policy changes that reduce exposure to heat, or improve people’s susceptibility and adaptivity to heat.
“By looking at emergency department visits for different causes and for several age groups, we were able to characterise with accuracy the varying impact on health on different populations,” said study co-author, Professor Francesca Dominici. “An important goal of this study is to provide actionable information to clinicians and public health experts regarding how to prevent these emergency department visits, also considering that we can anticipate when these extreme heat events are likely to occur.”
Researchers have uncovered differences in immune pathway activation to influenza infection between individuals of European and African genetic ancestry, according to a study published in Science. Many of the genes that were associated with these immune response differences to influenza are also enriched among genes associated with COVID disease severity.
“The lab has been interested in understanding how individuals from diverse populations respond differently to infectious diseases,” said first author Haley Randolph, a graduate student at the University of Chicago. “In this study, we wanted to look at the differences in how various cell types respond to viral infection.”
The researchers examined gene expression patterns in peripheral mononuclear blood cells, a diverse set of specialised immune cells that play important roles in the body’s response to infection. These cells were gathered from men of European and African ancestry and then exposed the cells to flu in a laboratory setting. This let the team examine the gene signatures of a variety of immune cell types, and observe how the flu virus affected each cell type’s gene expression.
The results showed that individuals of European ancestry showed an increase in type I interferon pathway activity during early influenza infection.
“Interferons are proteins that are critical for fighting viral infections,” said senior author Luis Barreiro, PhD, Associate Professor of Medicine at UChicago. “In COVID-19, for example, the type I interferon response has been associated with differences in the severity of the disease.”
This increased pathway activation hindered the replication of the virus more and limited viral replication later on. “Inducing a strong type I interferon pathway response early upon infection stops the virus from replicating and may therefore have a direct impact on the body’s ability to control the virus,” said Barreiro. “Unexpectedly, this central pathway to our defense against viruses appears to be amongst the most divergent between individuals from African and European ancestry.”
The researchers saw a variety of differences in gene expression across different cell types, suggesting a constellation of cells that work together to fight disease.
Such a difference in immune pathway activation could explain influenza outcome disparities between different racial groups; Non-Hispanic Black Americans are more likely to be hospitalised due to the flu than any other racial group.
However, these results are not evidence for genetic differences in disease susceptibility, the researchers point out. Rather, possible differences in environmental and lifestyle between racial groups could be influencing gene expression, and affecting the immune response.
“There’s a strong relationship between the interferon response and the proportion of the genome that is of African ancestry, which might make you think it’s genetic, but it’s not that simple,” said Barreiro. “Genetic ancestry also correlates with environmental differences. A lot of what we’re capturing could be the result of other disparities in our society, such as systemic racism and healthcare inequities. Although some of the differences we show in the paper can be linked to specific genetic variation, showing that genetics do play some role, such genetic differences are not enough to fully explain the differences in the interferon response.”
These differences in viral susceptibility may not be confined to just influenza. Comparing a list of genes associated with differences in COVID severity, the researchers found that many of the same genes showed significant differences in their expression after flu infection between individuals of African and European ancestry.
“We didn’t study COVID patient samples as part of this study, but the overlap between these gene sets suggests that there may be some underlying biological differences, influenced by genetic ancestry and environmental effects, that might explain the disparities we see in COVID outcomes,” said Barreiro.
As they explore this further, the researchers hope to figure out which factors contribute to the differences in the interferon response, and immune responses more broadly, to better predict individual disease risk.