Researchers have developed a new method to precisely and rapidly correct genetic alterations in cultured patient cells.
The genetically corrected stem cells are produced from a 2–3 mm skin biopsy taken from patients with different genetic diseases. The corrected stem cells are essential in the research and for the development of new therapies for the diseases in question.
The scientists based the new method on previous groundbreaking research in the fields of stem cells and gene editing; the first technique is the invention of induced pluripotent stem cells, iPSCs from differentiated cells, which won the Nobel in 2012. The other technique is the CRISPR-Cas9 ‘gene scissors’, which got the prize in 2020. The new method combines these techniques to correct gene alterations that cause inherited diseases, creating fully functional new stem cells.
The researchers aim to eventually produce autologous cells with therapeutic properties. The use of the patient’s own corrected cells could help in avoiding the immunological challenges hampering the organ and tissue transplantation from a donor. The new method was developed by PhD student Sami Jalil and is published in Stem Cell Reports.
More than 6000 inherited diseases are known to exist, which are caused by various gene alterations. Currently, some are treated with a cell or organ transplant from a healthy donor, if available.
“Our new system is much faster and more precise than the older methods in correcting the DNA errors, and the speed makes it easier and diminishes also the risk of unwanted changes,” commented adjunct professor Kirmo Wartiovaara, who supervised the work.
“In perfect conditions, we have reached up to 100 percent efficacy, although one has to remember that the correction of cultured cells is still far away from proven therapeutic applications. But it is a very positive start” Prof Wartiovaara added.
A new study from Karolinska Institutet in Sweden suggests that the early stages of sarcopenia, where muscles weaken with age faster than expected, could be counteracted with timely interventions designed to preserve physical and cognitive function and manage chronic conditions. The study’s findings are published in the Journal of Cachexia, Sarcopenia and Muscle.
Muscle mass and function is lost with ageing. When this decline is more extensive or rapid than expected, it is categorised as sarcopenia, a common condition in the elderly that often lowers quality of life and increases fall and fracture risks.
Researchers examined how different factors such as sex, age, educational level, living arrangement, lifestyle and chronic conditions affected the development of sarcopenia in people aged 60 and above across a 12-year period.
When the study began, almost 10% of the nearly 3200 participants had sarcopenia, 27% had probable sarcopenia and just over 63% no sarcopenia. Measurements such as grip strength, walking speed, speed of rising from a chair five times and calf circumference were used to assess muscle strength and mass and physical performance.
“Perhaps the most interesting result was that after five years, a roughly equal proportion (just over 10 percent) of the individuals with probable sarcopenia had either improved or deteriorated. This suggests that sarcopenia is a dynamic condition that is modifiable especially in the initial stages, which is a hopeful message,” said corresponding author Caterina Trevisan, affiliated researcher at the Department of Neurobiology, Care Sciences and Society, Karolinska Institutet.
Physical activity and higher results on cognitive tests improved odds of improvement and lowered mortality risk, while a higher number of chronic conditions, male sex and older age had the opposite correlation. For individuals initially diagnosed with severe sarcopenia, there was little chance of improvement, and many of them (almost 71%) died during the follow-up period.
“Our results support the need of early interventions to preserve physical and cognitive functions and manage chronic conditions in older individuals,” says the study’s last author Anna-Karin Welmer, senior lecturer at the Department of Neurobiology, Care Sciences and Society, Karolinska Institutet. “With these tools, we could probably counteract muscle deterioration and the impairment in quality of life this entails. We now need intervention studies to find ways to use these tools to counteract sarcopenia.”
Twenty years ago, clinicians first attempted to regenerate a failing human heart by injecting muscle myoblasts into the heart during a bypass operation. Despite high initial hopes and multiple studies since then, attempts to remuscularise an injured heart have met with little, if any, success.
Yet, there is hope that a therapy will be developed, according to experts in a Journal of the American College of Cardiology state-of-the-art review. The challenge is this: A heart attack kills heart muscle cells, leading to a scar that weakens the heart, often causing eventual heart failure. The lack of muscle repair is due to the very limited ability of mammalian heart muscle cells to proliferate, except during a brief period around birth.
In the review, the experts focus on three topics. First are several recent clinical trials with intriguing results. Second is the current trend of using cell-derived products like exosomes rather than muscle cells to treat the injured heart. For the third topic, authors discuss likely future experiments to replace a myocardial scar with heart muscle cells by ‘turning back the clock’ of the existing cardiomyocytes, rather than trying to inject exogenous cells. These efforts try to reverse the inability of mature mammalian heart muscle cells to proliferate.
Clinical trials One of the clinical trials reviewed involved giving cardiosphere-derived cells to patients with Duchenne muscular dystrophy, which affects both heart and skeletal muscles.
Cardiosphere-derived cells are a type of heart stromal/progenitor cell that has potent immunomodulatory, antifibrotic and regenerative activity in both diseased hearts and skeletal muscle. The HOPE-2 trial gave repeated intravenous doses of cardiosphere-derived cells to patients with advanced Duchenne disease, most of whom were unable to walk. Preliminary results showed safety, as well as major improvements in heart parameters such as left ventricle ejection fraction and reduced left ventricle size.
The HOPE-2 trial evaluated a repeated sequential dosing regimen of cell therapy for any cardiac indication, evaluated intravenous cardiosphere-derived administration, and clinically benefitted Duchenne patients.
Two features of the trial may bode well: a move away from invasive cardiac-targeted cell delivery and toward easily administered intravenous cell delivery, and the use of sequential repeated cell doses.
Cell-derived products Few cells transplanted into the heart survive, though some functional benefits in heart performance have been seen despite physical clearance of grafted cells. It could be possible that the cells were acting not as replacements but rather boosters of endogenous repair pathways through the release of a wide array of tissue-repairing biomolecules. This led to investigation of using cell-derived products rather than transplanting cells. Most of these biomolecules – proteins and non-coding nucleic acids – are enclosed in tiny vesicles that cells release naturally. When the vesicles, including exosomes, merge into recipient cells, the biomolecules can modulate signaling pathways. Using vesicles or exosomes involves a simpler manufacturing process compared with live cells, the ability to control quality and potency, and being able to refrigerate the vesicles to make administration simpler.
An alternative approach to the vesicle cell-derived products was the finding that injected stem cells can promote cardiac repair through release of biologically active molecules acting as short-range, paracrine hormones. These molecules are distinct from the biomolecules in vesicles or exosomes.
However, before use of any of these cell-derived products for heart repair in early trials, the reviewers say, more experiments are needed in purification of the products, potential modes of delivery and the suitability of repeated doses.
Proliferation of endogenous heart cells The final review topic looked ahead toward endogenous generation of cardiomyocytes – in other words, forcing existing native cardiomyocytes to divide, or other cells to become cardiomyocytes.
Pigs can regenerate heart muscle for only a few days after birth. But in one remarkable study, researchers injured the heart by removing part of the apex of the left ventricle one day after birth, and then induced heart attack 28 days after birth. Control pigs without the Day 1 resection showed no repair of heart attack damage at Day 56. In contrast, the pigs that had a resection one day after birth, and then had experimental heart attacks at Day 28, showed heart repair by Day 56 – notably an absence of dead heart muscle, known as an infarction. Furthermore, these pigs had more cardiomyocytes throughout their left ventricles.
This study showed that heart muscle cells in large mammals can be induced to proliferate and regenerate by inducing a heart injury at Day 1 to extend the neonatal regneration window. “If this cardiomyocyte cell-cycle activation can be activated in neonates, the same signaling pathways may be activated in adults as well,” the authors wrote, “which is highly impactful and significant.”
Another possible approach to endogenous generation is the direct programming of cardiac fibroblasts into cardiomyocytes. Inducing proliferation of cardiomyocytes will also need ways to promote growth of heart blood vessels to supply the new cardiomyocytes.
In conclusion, the authors believe that short-term approaches to clinical trials of post heart-attack therapies will use cells like cardiospheres or cell products. The longer-term approach, the reviewers said, will target “a more direct remuscularisation of the injured left ventricle by ‘turning back the clock’ of the cardiomyocyte cell-cycle or generating new cardiomyocytes from other cell types such as fibroblasts.”
“However, the efficiency and safety of these strategies, particularly their ability to generate cardiomyocytes seamlessly coupled with their native counterparts and to allow a regulation of these induced proliferative events preventing an uncontrolled and harmful cardiac growth, still need to be appropriately addressed before moving to clinical applications.”
University of Southampton researchers have found that the link between smoking at the start of pregnancy and having a smaller baby may extend to future pregnancies.
The research team studied data between 2003 and 2018 for nearly 17 000 mothers who received antenatal care for their first two pregnancies.
The findings, published in PLOS One, showed that, compared to non-smokers, women who smoked at the start of their first pregnancy were more likely to have a baby born smaller than expected in their second pregnancy. This held true even where they quit by the start of their second pregnancy.
The link between smoking during a pregnancy and that baby’s birth weight is well established. However, until now there has been limited evidence on the impact of maternal smoking on following pregnancies.
This study found that for women who smoked but did not smoke at the start of either pregnancy, there was no extra risk of a small for gestational age (SGA) baby in the second pregnancy compared to non-smokers. A mother who smoked ten or more cigarettes a day at the start of both of her first two pregnancies had the highest odds of SGA birth.
Study leader Dr Nisreen Alwan, Associate Professor at the University of Southampton, said: “It is important to encourage women to quit smoking before pregnancy and to not resume smoking after the baby is born. Resources that support mothers to quit and maintain smoking cessation are needed.”
First author Elizabeth Taylor said: “Women who smoke between pregnancies can reduce the risk of having a SGA baby by stopping smoking before the start of their next pregnancy. The period between pregnancies is when most mothers have close contact with health and care professionals and may require support to stop smoking.”
It is hoped that these findings and future research will encourage healthcare professionals and commissioners to provide better support to women before and between pregnancies, helping them to quit smoking, leading to better health for both mothers and children.
Saliva samples are easy to obtain and useful for measuring antibodies to SARS-CoV-2 in children, which could improve epidemiological surveillance in school settings. The study followed over 1500 children who went to summer schools in Barcelona last year. The results were published in BMC Medicine.
One of the pressing questions during this pandemic has been to understand children’s susceptibility to SARS-CoV-2 infection and how they infect others. An obstacle to answer this question is that most infections in children are mild or asymptomatic, and are therefore missed. To establish whether an individual has been exposed to SARS-CoV-2 in the past, virus-specific antibodies in blood need to be detected. Measuring antibody prevalence over time in a cohort of children can provide very valuable epidemiological information. However, this requires techniques that are both sensitive and minimally invasive.
In this study, performed through the Kids Corona platform, the team led by Carlota Dobaño, from the Barcelona Institute for Global Health (ISGlobal), and Iolanda Jordan, from Hospital Sant Joan de Déu (HSJD), used saliva instead of blood to measure virus-specific antibodies in over 1500 children who attended different summer schools in Barcelona in 2020, as well as around 400 adult staff. Two saliva samples per participant were analysed, one at the beginning and one at the end of the camp stay, and different antibody types (IgG, IgA and IgM) targeting different viral antigens were measured.
The study found that 3.2% of the participants developed antibodies between the first and second sample, indicating new infections. This is six times higher than the infection rate estimated by weekly PCR screening. “It has been reported that some children can be positive for antibodies despite being negative by PCR, which suggests that they can generate an immune response that prevents the establishment of SARS-CoV-2 infection,” explained Dobaño, first author of the study. It could also be because asymptomatic children have lower viral loads or that their viral clearance is faster.
Furthermore, the analysis shows that the percentage of new infections was higher in adults (2.94%) than in children (1.3%), suggesting differences in infection and transmission dynamics. Finally, contrary to blood tests, asymptomatic people had higher levels of anti-Spike antibodies in saliva, suggesting these antibodies play a protective role in respiratory mucosae. “This means that anti-Spike antibodies in saliva could be used to measure protective immunity upon vaccination, especially in the case of intranasal vaccines,” said senior study co-author Gemma Moncunill.
“We previously demonstrated in other Kids Corona studies that saliva is useful for detecting virus by PCR. With this study, we demonstrate that it’s also an effective and much friendlier way to measure antibodies, making it the ideal sample for children, instead of the more invasive nasal swab,” said Jordan.
Older women are more likely to struggle with both regular daily tasks and mobility activities, according to new analysis of longitudinal cohort studies.
However, the researchers say disparities in ability to perform daily tasks have been steadily decreasing as the socioeconomic gap between the sexes has decreased.
The international study, published in The Lancet Healthy Longevity, uses data from more than 27 000 men and 34 000 women aged 50 to 100, born between 1895 and 1960, to examine sex differences in daily activity and mobility limitations. Researchers at UCL and the National Institute of Health and Medical Research (INSERM) in France drew on four large longitudinal studies, covering 14 countries*.
Women were more found to be more likely than men to be limited in their ‘functional capacity’ (both tasks and mobility) as they get older. From age 75, women were also more likely to have three or more mobility issues (such as going up a flight of stairs) or limitations with more complex daily tasks (eg managing money) compared to men who were more likely to have just one or two. At age 85 years, the prevalence of three or more mobility limitations was 10% higher in women than in men.
Lead author, Mikaela Bloomberg, UCL PhD candidate, explained: “Our study of over 60,000 participants born between 1895 and 1960 provides new insights on functional limitations and sex differences.
“We found that women are more likely to be limited than men in carrying out daily tasks from age 70, while we observed women were more likely to be limited in mobility activities from age 50 onward.
“This is an important observation because mobility limitations can precede other more severe limitations and targeting these gaps at middle age could be one way to reduce sex differences in limitations at older ages.”
Historical socioeconomic differences between men and women in areas such as education and entrance to the labour force may partly explain these differences, as women are disproportionately exposed to associated health risks that can lead to disability.
“It appears that gender inequalities in the ability to carry out daily tasks at older age are decreasing over time and this could be explained by the fact that women have better access to education and are more likely to enter the paid labour force in recent generations,” said Bloomberg.
“And although reductions in socioeconomic inequalities may be associated with smaller disparities in simple daily tasks, we did not see the same reductions in sex disparities for mobility after accounting for socioeconomic factors. This might be partly due to sex differences in body composition such as body mass and skeletal muscle index but more research is needed to identify other factors.”
Co-author Dr Séverine Sabia added: “Developing targeted prevention policies to preserve independent living and quality of life for older adults requires an understanding of drivers of sex differences in functional limitations.
“Our study indicates improvements in socioeconomic conditions for women could play an important role in reducing these sex differences. Findings also highlight the importance of early prevention to tackle sex differences in mobility that may trigger sex differences in disability at older age.”
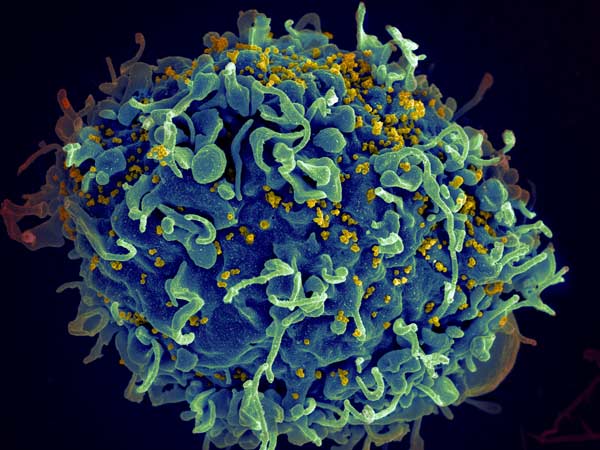
Researchers examining the development of resistance to HIV drugs have uncovered a mechanism of drug resistance development in combination therapy, where ‘windows’ open up for resistance to develop.
In the late 1980s, when HIV treatments were first introduced, patients would often develop resistance to those treatments within six months. The introduction of triple-drug treatment regimens in the 1990s was intended to rectify that. Even if the virus developed resistance to one drug, two others would still knock it out – in theory. Unfortunately, some patients still develop resistance, leaving scientists with a critical question to answer: Why?
“There’s all these things that we still don’t understand, like why do we even get resistance when treating with three drugs,” said San Francisco State University Associate Professor of Biology Pleuni Pennings. “We understand why it is becoming less common, but it should have been zero all along.”
Prof Pennings and her colleagues offer explanations for this phenomenon in a study published in eLife.
Several interesting observations were noted from analysis of HIV patient records. Drug resistance can evolve years after successful therapy, often the result of sequential mutations that occur in a predictable order. Current models could not explain these observations, and while some studies identify mutations that confer drug resistance, they don’t address how and where they arise.
Drawing on two computational models, the researchers suggest that these observations may result from drug heterogeneity over time and throughout the body. While patients receive three HIV therapies simultaneously, drugs have different half-lives and patients do not always adhere to therapy regimens. This could create opportunities for drug resistance evolution, during a window when only one drug is active. Drugs also don’t uniformly penetrate the entire body, meaning that in some locations in a patient’s body, only one of the drugs might be active, creating another evolution and escape opportunity.
“I think one main reason why we should care is actually not because of HIV but because of drug resistance in other situations,” Prof Pennings explained.
Although drug resistance among patients with HIV is fairly low, drug resistance to multidrug therapies is a big problem for diseases such as malaria and tuberculosis. In addition, the COVID pandemic and the rise of variants show how our understanding of evolving pathogens is still lacking.
“In a way, HIV is the poster child of how we solved drug resistance. … [But] if we don’t understand how we did it, then it’s really hard to take these lessons to other situations,” Prof Pennings said.
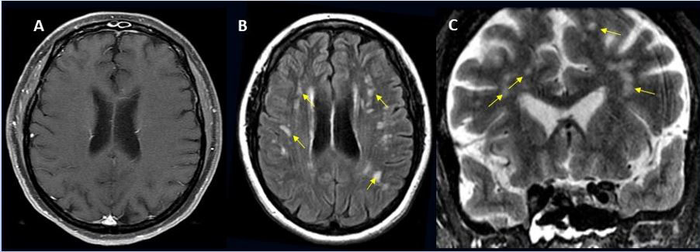
49-year-old female with past medical history of mitral valve disease and tricuspid valve regurgitation who developed headache followed by cough and fever presented to the ER with right upper eyelid ptosis (drooping). Credit: Radiological Society of North America and Scott H. Faro, M.D.
Approximately one in 100 patients hospitalised with COVID will likely develop complications of the central nervous system, according to a large international study. These can include stroke, haemorrhage, and other potentially fatal complications. The study was presented at the annual meeting of the Radiological Society of North America (RSNA).
“Much has been written about the overall pulmonary problems related to COVID, but we do not often talk about the other organs that can be affected,” said study lead author Scott H. Faro, MD, FASFNR, professor of radiology and neurology at Thomas Jefferson University. “Our study shows that central nervous system complications represent a significant cause of morbidity and mortality in this devastating pandemic.”
Dr Faro initiated the study after finding that only a small number of cases informed existing literature on central nervous system complications in hospitalised COVID patients.
To build a more complete picture, he and his colleagues analysed nearly 40 000 cases of hospitalised COVID patients, admitted between September 2019 and June 2020. Their average age was 66 years old, and two thirds were men.
Confusion and altered mental status were the most common causes of admission followed by fever. Comorbidities such as hypertension, cardiac disease and diabetes were common.
There were 442 acute neuroimaging findings most likely associated with the viral infection, with central nervous system complications in 1.2% of this large patient group.
“Of all the inpatients who had imaging such as MRI or a CT scan of the brain, the exam was positive approximately 10% of the time,” Dr Faro said. “The incidence of 1.2% means that a little more than one in 100 patients admitted to the hospital with COVID are going to have a brain problem of some sort.”
Ischaemic stroke, with an incidence of 6.2%, was the most common complication, followed by intracranial haemorrhage (3.72%) and encephalitis (0.47%).
A small percentage of unusual findings was uncovered, such as acute disseminating encephalomyelitis, an inflammation of the brain and spinal cord, and posterior reversible encephalopathy syndrome, a syndrome that mimics many of the symptoms of a stroke.
“It is important to know an accurate incidence of all the major central nervous system complications,” Dr Faro said. “There should probably be a low threshold to order brain imaging for patients with COVID.”
The emergence of the Omicron SARS-CoV-2 variant which has resulted in renewed lockdowns and travel bans around the world, which have been criticised by the WHO. In contrast, South Africa will stick to an adjusted Level 1 lockdown for the time being, though pushing for mandatory vaccinations. Business and civil society groups had warned that increasing restrictions would have provoked backlash as recent election campaign events had effectively ignored them.
Many nations around the world have reacted quickly to the new variant, which has a large number of mutations compared to the Delta variant. The UK’s decision to suspend flights from South Africa as well as nine other African countries has provoked criticism from a number of quarters, including President Cyril Ramaphosa. The sudden move has caught many travellers by surprise, including a Welsh rugby team which had two members test positive, one of which was for Omicron. They will have to self-isolate before they are able to return, depending on flight availability.
Japan and Israel have taken the more extreme steps of closing their borders to foreigners. The first cases of Omicron that were recorded in Botswana were revealed to be in visiting diplomats, although which country they came from has not been revealed.
The World Health Organization criticised the imposition of travel restrictions, acknowledging that although they may play a role in slightly reducing the spread of COVID, they still place a heavy burden on lives and livelihoods. It pointed out that if restrictions are implemented, they should not be unnecessarily invasive or intrusive, and should be scientifically based, under international law, the International Health Regulations. It notes South Africa followed International Health Regulations, and informed WHO as soon as its national laboratory identified the Omicron variant.
“The speed and transparency of the South African and Botswana governments in informing the world of the new variant is to be commended. WHO stands with African countries which had the courage to boldly share life-saving public health information, helping protect the world against the spread of COVID,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “On the eve of a special session on pandemic preparedness I urge all countries to respect their legal obligations and implement scientifically based public health actions. It is critical that countries which are open with their data are supported as this is the only way to ensure we receive important data in a timely manner.”
Although a full picture of the new variant’s severity is still two or three weeks away, Angelique Coetzee, chair of the South African Medical Association, told the AFP she had recently seen around 30 patients at her Pretoria practice who tested positive for COVID but had unfamiliar symptoms.
“What brought them to the surgery was this extreme tiredness,” she said, something she said was unusual for younger patients. Most were men under 40, and just under half were vaccinated. Other symptoms included mild muscle aches, a “scratchy throat” and dry cough, she said. Just a few had a slightly high temperature. These very mild symptoms stand in contrast to other variants, which typically result in more severe symptoms.
Viral RNA levels in the blood is a reliable indicator in predicting COVID mortality, according to a study published in Science Advances.
“In our study, we were able to determine which biomarkers are predictors of mortality in the 60 days following the onset of symptoms,” said Université de Montréal medical professor Dr. Daniel Kaufmann, the study’s co-lead author alongside colleagues Nicolas Chomont and Andrés Finzi.
“Thanks to our data, we have successfully developed and validated a statistical model based on one blood biomarker,” viral RNA, Prof Kaufmann said.
Despite advances in COVID management, identifying patients at greater risk of dying of the disease has been difficult. Other studies identified various biomarkers, but assessing so many parameters is not possible in a clinical setting and gets in the way of doctors’ quick clinical decision-making ability.
Using blood samples from 279 patients hospitalised for COVID of differing severity, Kaufmann’s team measured amounts of inflammatory proteins, looking for any that stood out.
At the same time, Chomont’s team measured the amounts of viral RNA and in Finzi’s the levels of antibodies targeting the virus. Samples were collected 11 days after the onset of symptoms and patients were monitored for a minimum of 60 days after that.
The goal: to test the hypothesis that immunological indicators were associated with increased mortality.
“Among all of the biomarkers we evaluated, we showed that the amount of viral RNA in the blood was directly associated with mortality and provided the best predictive response, once our model was adjusted for the age and sex of the patient,” said Elsa Brunet-Ratnasingham, a doctoral student in Kaufmann’s lab and co-first author of the study.
“We even found that including additional biomarkers did not improve predictive quality,” she added.
Prof Kaufmann and Brunet-Ratnasingham tested the model on two independent cohorts of infected patients from Montreal’s Jewish General Hospital (recruited during the first wave of the pandemic) and the CHUM (recruited during the second and third waves).
No matter which hospital the patients were treated at, nor which period of the pandemic they fell into: in all cases, the predictive model worked. Now Prof Kaufmann and his colleagues want to put it to practical use.
“It would be interesting to use the model to monitor patients,” he said, “with the following question in mind: when you administer new treatments that have proven effective, is viral load still a predictive marker of mortality?”